- Laparoscopic Mesh Repair of Inguinal Hernia
- Femoral Hernia Repair
- Mesh Repair of Umbilical and Paraumbilical Hernia
Laparoscopic Mesh Repair of Inguinal Hernia
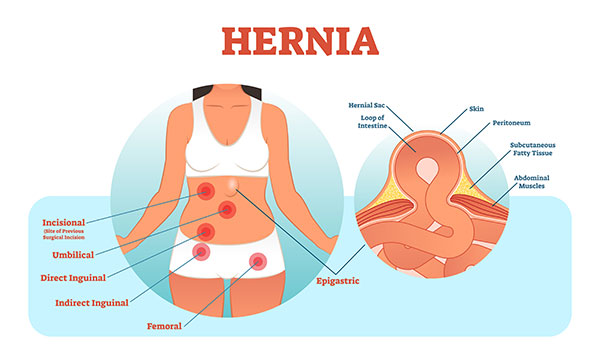
A hernia occurs when the internal organs of the abdominal cavity push through a weakened spot in the abdominal wall to form a bulge. Hernias occur most commonly between the area of your rib cage and groin.
Hernias may be repaired surgically by closing the defect and using mesh to strengthen the weakened area. This can be performed in a minimally invasive manner using a laparoscope.
Dr Toshniwal is highly experienced in laparoscopic total extraperitoneal (TEP) surgical technique for inguinal, femoral & spigelian hernia repairs. The advantage of this technique is that it prevents the risk associated with damage to the internal organs as it is performed outside of the peritoneum. Please click on the Patient Info link below for more information. You can also view a comparison of surgical techniques for inguinal hernia repair here
Femoral Hernia Repair
A hernia occurs when the internal organs of the abdominal cavity push through a weakened spot in the abdominal wall to form a bulge. Hernias occur most commonly between the area of your rib cage and groin.
Hernias may be repaired surgically by closing the defect and using mesh to strengthen the weakened area. This can be performed in a minimally invasive manner using a laparoscope.
Mesh Repair of Umbilical and Paraumbilical Hernia
An umbilical or paraumbilical hernia is a weakness in the abdominal wall at or near the navel through which the contents of the abdomen protrude to form a bulge.
Dr Sumeet Toshniwal - Groin Hernia Surgery Comparison
| Open Hernia Surgery | Laparoscopic Hernia Surgery | Total Extraperitoneal Hernia Surgery | |
| Surgery Summary | |||
| About | Most common technique used for hernia repair. | Less common approach for hernia repair. | Most advanced technique. Suitable for unilateral, bilateral and recurrent hernias repair. |
| Suitable For | Elderly people or any patient not eligable for Laparoscopic / Extraperitonal Repair (eg: unable to have general anaesthesia) | Suitable for patients who have had previous robotic prostatectomy or an hysterectomy | Suitable for all patients except patients ineligible for general anaesthesia or ineligible for open lower abdominal surgery |
| Obese Patients | Less suitable for obese patients as more invasive, with larger incision and surgical dissection | More suitable for obese patients as the procedure is less invasive and requires less surgical dissection | Most suitable for obese patients as the procedure is less invasive and requires less surgical dissection |
| Surgical Overview | |||
| Benefits | Common experience, widely available. And is used for some large, chronic, long standing hernias can be difficult to repair. | Keyhole procedure, preserves structure of the muscle tissue, less invasive, faster recovery | Least invasive, less pain both post operative and long term chronic nerve pain due to less muscle and nerve damage. Lower rate of hernia recurrence. Quicker return to normal activities (e.g. Work, sport etc) |
| Disadvantages | Most invasive procedure. Increased postoperative pain from muscle and nerve damage. Higher rate of hernia recurrence. Slower return to normal | Higher risk of adhesion and bowel injury than Total Extraperitoneal Hernia Surgery | Only disadvantage are the normal risks associated with surgery |
| Surgical Duration | Surgery is usually about 30-45 minutes in length. | Surgery is about 45-60 minutes in length. | Surgery requires more time approx 60+ minutes in duration |
| Skill Level | Very common with significant variation in surgical techniques and outcomes | Requires advanced experience and laparoscopic surgery skills | Requires the highest level of Hernia repair skills. |
| Fee Comparison | Most cost effective option for Self-Funded patients. | Higher costs for Self-Funded patients due to the additional laparoscopic equipment needed. | Higher costs for Self-Funded patients due to the additional laparoscopic equipment needed. |
| Surgical Preparation | Basic preoperative workup is required. | Occasionally requires more advanced workup because general anesthesia is used. | Occasionally requires more advanced workup because general anesthesia is used. |
| Surgical Requirement | Standard surgical equipment. | Advanced laparoscopic equipment. | Advanced laparoscopic equipment. |
| Surgery Details | |||
| Method | Surgery involves folding away the tissue and muscle layers to access a herniated tissue underneath | This procedure uses a small keyhole Incision using minimally invasive surgery but uses a peritoneal incision that requires stitching. | Method involves no muscle dissection and considerably less local trauma or peritoneal stitching |
| Surgical Approach | Hernia is fixed by opening the muscles over the weakness. | Hernia is fixed from the inside, behind the muscles where the weakness is located. | The most anatomical repair as it matches the natural anatomy |
| Mesh Placement | Mesh is placed behind the muscle and above the muscle. The mesh is sutured in place. | The peritoneum is cut, the mesh is placed between the peritoneum and the muscle. The mesh is secured in place with absorbable sutures. | This method involves no peritoneal dissections staying behind the muscle and in front of the peritoneal sac and the mesh is placed between the two |
| Type of Mesh Used | Traditionally a heavier prolene mesh is used | Lightweight mesh. Less scarring, pain and post op infection | Lightweight mesh. Less scarring, pain and post op infection |
| Access to the Hernia | 4-5 cm incision in the groin or bikini area. | 1-2 cm incision next to the belly button, and 2 small punctures below the belly button. | 1-2 cm incision next to the belly button, and 2 small punctures below the belly button. |
| Procedural Anesthesia | Can be done under local or spinal anesthesia with sedation. | Requires complete general anesthesia. | Requires complete general anesthesia. |
| Completing the procedure | Surgeon sutures required to close the surgical area | Small the port hole closed with tape | Small the port hole closed with tape |
| Recovery from Surgery | |||
| Post Op Pain | On average, 1/3 of patients have little to no pain after surgery. 2/3 have moderate pain post op. | Less Pain - on average, 2/3 of patients have little to no pain after surgery. 1/3 have moderate pain post op. | Less Pain - on average, most patients have any discomfort after surgery. Some develop temporary bruising around lower abdomen |
| Potential complications | Possible chronic pain, numbness and infection. | Possible postoperative adhesions and bowel injury | Rare possibility of injury to major blood vessels |
| Infection Rates | Highest | Low | Very Low |
| Bandage | Bandage and drainage for 3 weeks after surgery | Local area recover within 1-2 weeks after surgery | Local area recover within 1-2 weeks after surgery |
| Healing | Variable post op outcomes. In some incidences patients suffer discomfort and movement restrictions | Patients most experience a quick return to normal, with little post op discomfort or movement restrictions | Patients most experience a quick return to normal, with little post op discomfort or movement restrictions |
| Activity restrictions | Most patients will return to normal activities within 3-6 weeks. However post-operative activity restrictions apply for heavy lifting with a gradual return to normal activities over 6-12 weeks. |
Most patients will return to normal activities within 1-2 weeks.
However post-operative activity restrictions apply for heavy lifting with a gradual return to normal activities over 6-12 weeks. |
Most patients will return to normal activities within 1-2 weeks. However post-operative activity restrictions apply for heavy lifting with a gradual return to normal activities over 6-12 weeks. |
| Recurrence Rates | Highest | Low | Very Low |
| Groin Hernia Surgery Comparison | |||